
Athletes around the world are often plagued with snapping hip syndrome. It’s a condition that doesn’t always cause pain, but it can cause discomfort along with it’s notable ‘snapping’ sound during a movement. It’s not a fully understood condition, which means the best treatment option is not always apparent. In many cases it can exist for many years in an athlete.
This is a very common Hip Flexor injury, especially to dancers, which is why it’s sometimes called ‘dancer’s hip’. It’s been reported that over 90 percent of ballet dancers develop it at one time or another in their careers, and often are forced to train and perform through it [1].
What Causes Snapping Hip Syndrome?
The root cause of the syndrome is a ligament or tendon snapping over a part of the hip, not unlike snapping an elastic band over your finger. The tricky part is identifying the exact location of the issue and the structures involved. The continuous snapping typically occurs during a specific type of movement, usually something to do with raising a leg, and can potentially lead to inflammation or other pain in the Hip Flexors in the future. It is often associated with Hip Flexor tendonitis as well.
Types of Snapping Hip
There are actually three types of this syndrome that in order to identify you will need to see a physician; even then it’s not always easy to find [2].

-
External: This is the easiest type to diagnose and is also the most common. It usually involves the iliotibial band (ITB) or the anterior gluteus maximus (the frontal portion) snapping over the greater trochanter of the femur when the hip is flexed. This is very common in cyclists or runners, who also frequently experience ITB syndome [3].
-
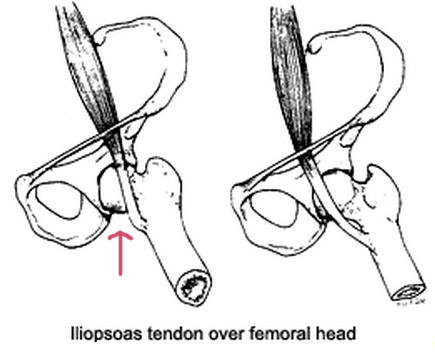
Internal: Not fully understood, but caused mainly by the Iliopsoas tendon or Iliofemoral ligament snapping over the lesser trochanter or femoral head [4].
-
Intra-articular (joint): This third type refers to damaged ligament or out of place fractures causing the snapping sound, but this is far less common than either of the other types.
How to Identify the Syndrome
Snapping caused by the ITB (external) in particular can often be found with this simple test:
-
Lie on your side
-
Move your leg through a complete range of hip flexion, starting by extending is straight back and then going forwards. Listen for a snap or any pain. Preferably find someone to move your leg through this motion.
-
If there were no issues with step 2, go through external and internal rotation. This means turning your foot outwards and inwards with a relatively straight leg.
To test for the most common internal type, caused by the Iliopsoas tendon, perform the following:
-
Lie on your back with the unaffected leg lying straight out.
-
Bring and bend your other leg across just above your knee, the knee of the bent leg should be facing out to the side.
-
Have someone move your leg so your hip is extended (gently pushing down on bent leg), adducted (coming across your body) and internally rotated. Listen for the snap and notice any pain that might indicate the syndrome.
If you do happen to have an intra-articular case, you will most likely need diagnostic imaging to identify the issue.
Snapping Hip Syndrome Treatment Options
While you may be able to continue training and performing activities without any pain, there are some treatment options available.
Professional athletes, when faced with the sydrome and pain have had positive results using myofascial release on the psoas muscle when done at least twice a week for a short time period [5]. A sports massage therapist should be able to provide this specific technique. You can also attempt it on your own by using a foam roller.
If these non-intrusive options do not help, the last resort is a surgical one.
Surgical Treatment
When all else fails, there is almost always a surgical option. While open surgery has been successful in the past, there have been very promising results with arthroscopic surgery for internal snapping hip syndrome cases [6]. An arthroscope is a small camera which allows for any work done to be completed through just a small incision, often less than a centimeter. The picture below is what a surgeon would see through the arthroscope.
%2C_and_the_lower_the_high-speed_burr_(for_reshaping_the_bone)..png)
The surgeon will attempt to release the Iliopsoas tendon at the level of the lesser trochanter. The results of one study of four cases where this procedure was followed showed that all symptoms were fixed immediately after surgery and again at the 21 month follow-up appointment. Note that if you do end up going with an option like this, you will experience a decrease in hip flexion strength for up to 8 weeks.




{kind=link}